Hi all,
This morning I finally had a chance to listen to our debate in Amsterdam from 9th January. And I find that we are not that far apart on some points, though we remain in opposite corners on others. When I posted the slides from my talk and described the evening’s dialogue, my impression was that I was taking on the disease model as a sort of David fighting Goliath (a handy form of grandiosity when you’re the weakling). And while we did and do clash swords at times, maybe that’s only half the story.
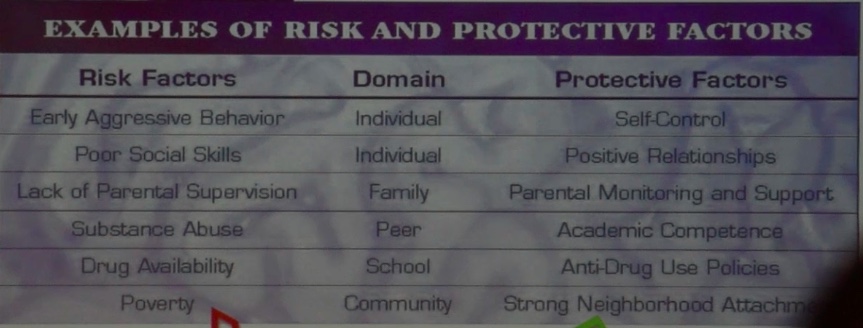
One of Nora Volkow’s slides
What does it signify that Nora Volkow talked explicitly about the power of the social environment, the role of stress in triggering relapse, the risk created by growing up poor, with inadequate parental monitoring? What about her emphasis on the value of positive social relationships and support? Her clear (and to my ears novel) discussion of recovery, of the fact that many one-time addicts get over it — for good — which seems a far cry from NIDA’s characterization of addiction as a chronic disease? In fact Nora showed a slide depicting how social subordination (at least in monkeys) 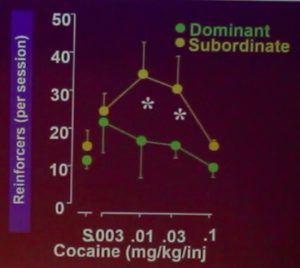 greatly increases vulnerability to addiction — and the brain mechanics that might underlie this relationship. It was a slide I might have used myself, as it identifies addiction as a response to low self-esteem, isolation, and/or frustration — a point that Carl Hart or Johann Hari or I might just as easily have made.
greatly increases vulnerability to addiction — and the brain mechanics that might underlie this relationship. It was a slide I might have used myself, as it identifies addiction as a response to low self-esteem, isolation, and/or frustration — a point that Carl Hart or Johann Hari or I might just as easily have made.
What I think it shows is that Nora Volkow is talking about addiction in a broader light than ever before, paying homage to the social, psychological, and even societal forces that get people to take drugs. And maybe it shows that Nora Volkow can lead NIDA and similar organizations into a more evolved understanding of addiction, rather than serve as an anchor that holds the disease model in place. In fact — and this is purely speculation — maybe Nora finds herself between a rock and a hard place, trying to balance the pathology-oriented brain data (and the research program that spawns it) against insights that are sensitive, humanistic, and true to the actual experience and context of addiction in our society. And/or maybe Stanton Peele, Bruce Alexander, Maia Szalavitz, Carl Hart and others (like me) have been nipping at her heels to some effect.
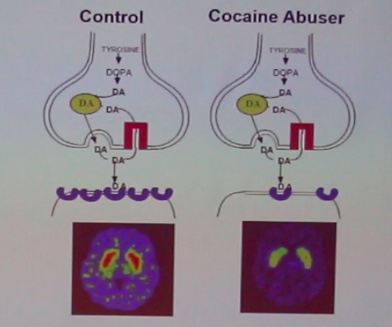 She and I still have our differences of course. I can’t stand her slides showing big red or yellow splotches on the brain scans comparing cocaine addicts to “normals”. She and her colleagues certainly know that cocaine and other psychostimulants compile dopamine in the synapses, unlike the many other addictive drugs that do no such thing, which could easily explain a temporary blunting of dopamine metabolism as a compensation. Yet she points to those slides and says: see, look how different their brains are. Not fair! And she still talks about addiction as destroying will power, which still seems to me entirely wrong-headed (though that’s sometimes how it seems). And then I wonder, is that her talking, or is that the NIDA party line? And if it’s the latter, then maybe she really is walking a kind of professional tightrope or perhaps struggling with her own intuitions while trying to be a good scientist. I know that feeling myself.
She and I still have our differences of course. I can’t stand her slides showing big red or yellow splotches on the brain scans comparing cocaine addicts to “normals”. She and her colleagues certainly know that cocaine and other psychostimulants compile dopamine in the synapses, unlike the many other addictive drugs that do no such thing, which could easily explain a temporary blunting of dopamine metabolism as a compensation. Yet she points to those slides and says: see, look how different their brains are. Not fair! And she still talks about addiction as destroying will power, which still seems to me entirely wrong-headed (though that’s sometimes how it seems). And then I wonder, is that her talking, or is that the NIDA party line? And if it’s the latter, then maybe she really is walking a kind of professional tightrope or perhaps struggling with her own intuitions while trying to be a good scientist. I know that feeling myself.
 I quite like this woman. Her very expressive face (sometimes pleasant, sometimes fierce) is currently looking up at me from the cover of LEF magazine, a Dutch publication for addicts and those who live or work with them. I admire her energy and her devotion to data, not to mention the heap of accomplishments she’s contributed as an active neuroscientist — regardless of or despite her role as the head of NIDA. So I’ll end with a paragraph from an email I just sent her.
I quite like this woman. Her very expressive face (sometimes pleasant, sometimes fierce) is currently looking up at me from the cover of LEF magazine, a Dutch publication for addicts and those who live or work with them. I admire her energy and her devotion to data, not to mention the heap of accomplishments she’s contributed as an active neuroscientist — regardless of or despite her role as the head of NIDA. So I’ll end with a paragraph from an email I just sent her.
Hi Nora,
I finally had a chance to listen to the recording made that evening in Amsterdam. I want to say that I have now really listened to your words, and I see that our perspectives are getting more and more convergent. Your emphasis on environmental factors, on the importance of social support in recovery, your discussion of diversity in outcomes…so many things we actually agree on. And of course we also agree (and I acknowledged) how important it is to stop blaming and start helping. I feel a bit guilty, partly because you were so tired that night — I thought it was heroic that you spoke so energetically and clearly after three days of meetings and talks..and jet lag — but also because my main points were critical of the traditional disease model, and maybe I didn’t acknowledge how much your thinking seems to be increasingly comprehensive, and how much common ground we can find.
 Informed by unparalleled neuroscientific insight and written with his usual flare, Marc Lewis’s The Biology of Desire effectively refutes the medical view of addiction as a brain disease. A bracing and informative corrective to the muddle that now characterizes public and professional discourse on this topic.” —Gabor Maté, M.D., author of In The Realm of Hungry Ghosts: Close Encounters With Addiction
Informed by unparalleled neuroscientific insight and written with his usual flare, Marc Lewis’s The Biology of Desire effectively refutes the medical view of addiction as a brain disease. A bracing and informative corrective to the muddle that now characterizes public and professional discourse on this topic.” —Gabor Maté, M.D., author of In The Realm of Hungry Ghosts: Close Encounters With Addiction
This is so refreshing! As humans, slathering labels onto stuff is how we make sense of the world and navigate our reality. Sometimes the seemingly far afield differences are just differences in perspective and have more in common than not.
It’s very interesting how we can get caught up into semantics and perhaps have a strong desire to be Right! I believe it was John Bradshaw who said, and he was quoting someone else, “Whenever you think you are right, you’ve killed your creativity”. A person who thinks they are absolutely right narrows their vision to such a degree that there isn’t any room for any other possibility.
However, the other interesting thing in both your cases, from my own point of view, is just how passionate you both are inevitably for the same cause.
Perhaps there is something that can only exist between you and Nora in that its not what you bring or what she brings but the awareness in-between. On the other side of the experience there isn’t any ownership just pure awareness, love and appreciation for just cause. This is possibly is what makes us most human the ability to acknowledge the otherness without judgment.
In my days of addiction counseling listening helped so much more than speaking. I also realized that what causes a problem is a problem regardless if one is addicted due to disease, learned behavior or otherwise. Although, for me, in my own addiction, I realized the impact and influence the chief components in my family had on me due to their behavior and/or substance abuse. It’s like passing a baton from generation to generation causing one to think it’s biological in nature while the modeling gets carried over.
So! in many respects, we learn the good, bad and the ugly. Once we become aware, it is then we become responsible to change not blame!~
I think the ego-driven, intrinsic need to be right comes not so much from that per se, but from the very adaptive distaste for being wrong. If I am wrong about something important, I am potentially vulnerable and in danger.
This comes into play in the societal ignorance and willful stupidity about addiction and thus the backwards-ass approaches to recovery that ensue. Often these approaches are characterized by prescriptive, one-size-fits-all methods, as if for a hangnail and not the human condition. A major potential problem with the disease model is not just that it overmedicalizes addiction. It oversimplifies it, and thus gives short shrift to the multifactorial nature of its development as a compulsive, reactive coping adaptation to stress. Dr. Volkow seems to be taking more of these varied “etiological” factors into consideration, which is encouraging. But she still makes simplistic pronouncements such as addiction destroying willpower. If that were true, not only would it be very difficult to maintain an addiction, but nobody would ever be able to recover either, and people do it all the time.
I wonder if a play-on-words, similarly, is intrinsic in terms of stroking the ego as well. Much like a gambler who perhaps plays the Slots, when they put money into the machine in order to “feel like a winner” versus losing and thus “feeling like a loser. “Recovery” has its own limitations also, in my own opinion. One can never “recover” that which they never had in the first place, however, they may in fact “discover” things about themselves for the first time. Addiction may not “destroy” will power but perhaps give the illusion that ones’ willpower and/or “choice” is absent.
Interpretation plays a vital role in ones’ understanding, hopefully, through respectful meaningful dialogue there comes a meeting of the minds where nobody is “right” or perhaps “wrong”. They are just in different places in their view and/or conditioning.
Absolutely. “Recovery” is part of the overmedicalized term that’s the one everyone uses when referring the dually crappy designations of “addiction” and “recovery”. What happens is people “rehabituate” to a more fulfilling, rewarding, validating habit. They don’t go back to, or get back anything. They navigate change. I habituated to the “secret” reward of my addictive behavior because I didn’t believe I deserved any better. That’s what I learned growing up…how to devalue myself. It took a lot of evidence to the contrary to convince me otherwise, which did not change my negative interpretation… my belief… that I’m a bad person. Subjective belief is not rational, but I have to start with that as the foundation, and build evidence on top of that to the contrary. The reason I, and many, use maladaptive behaviors to cope is because I got a very strong message that I was not worthy of any better at a very pivotal age. It may be an illusion (as all this is, in my opinion), but when you are backed into a corner without being aware of options, “choice” is absent for all intents and purposes. There is very little “truth” that is not subject to interpretation, and when beliefs are imposed on the weak or vulnerable, people find ways to adapt and survive with what they have to work with.
Hi Matt,
Regarding your comment…this is a place where I can, without question, relate!~
A meeting of the minds or perhaps souls!~
Thank You!~
Matt, Gary, I think research will also show that a large percentage of people that regain their dependency from an addiction, (i.e. recover), look back and consider the period of addiction was a diversion from their original self & interests, rather than changing, or “rehabituating” to more fulfilling, rewarding, validating habits.
For instance, years ago, a SMART Facilitator expressed concern that his original nature of being rather “Snarky” was returning, and was concerned he was not representing SMART, or even the Recovery process properly.
We talked about it, and came to the conclusion that the facilitator’s authenticity was more valuable than a specified or learned way of Facilitating.
I think a major reason many people don’t return to an addiction is because it no longer delivers a feeling of freedom from the traumas and pains of life.
In effect, the addiction became an extra burden and distraction from one’s original sense of life.
Getting something back, your own authentic self, which seemed lost forever, then becomes very deeply valued.
Hi Carlton,
In my own opinion, whatever one might deem to be the “authentic self” can never be lost or perhaps even “known”, again, in my own opinion. The initiation, if you will, with respect to addiction, doesn’t always happen as a result of trauma and/or pain. I believe for many curiosity, peer-pressure, modeling etc., play a significant role.
Attachment too and/or the illusory sense of knowing ones’ self can in fact be part of the problem. Example, “who I am”, is one who drinks, smokes, gambles, or labels themselves alcoholic, drug addict or social roles at work…
I once heard spoken, “the greatest act you’ll ever achieve is the act of being yourself”. Again, “an act”.
The wonder of the world has little to do with act or action as much as it has to do with being and awareness. Awareness without a reference point manifests an alignment beyond the thinking brain which is limited.
There is no method or model or act, or as Jiddu Krisnumarti said “There is no path to truth” or to that which is sacred if conjured up by ones’ mind.
Gary, I am still trying to find the best words to describe what was experienced.
Thanks for pointing out how “authentic self”
simply has too many facets to it 🙂
Here here. All we can do is change habits from negative self defeating behaviours to positive habits based on a more caring and realistic view of ourselves denying the messages from youth that affected the formation of the individuals personality. You can’t rehabilitate a person who was never habilitated in the first place and you can’t remove habits and leave nothing there. Drug, set and setting.
Terry:
You definately are one of the many voices I enjoy hearing from on this blog! I appreciate your input.
I know you’ve spoken of this before but Could you again explain “You can’t rehabilitate a person who was never habilitated in the first place.” and how are you applying this to Drug, set and setting?
Hi Carl. Initially I feel drugs are used to help confidence in particular in regards to relationship with others, in the transition from youth to adulthood; initially friends and the other sex (or same). The high anxiety fuelling this in the susceptible individual means they quickly see the success of this coping mechanism and then begin to use drugs (and alcohol and other behaviours) to cope on a broader scale and in doing so do not develop other, in the long run more effective, ways to cope with ‘life”. That means they are not ‘habilitated “in the sense that they do not have to the skills to go back to when “rehabilitation” occurs rather they have to learn ‘new’ skills. More and more I see addiction as learned behaviour and change as being both an unlearning of old ways and a new learning of new ways. This fits in as both related to the set, the inner workings of an individual and the setting, the less helpful relationships developed in the negative addiction coping mechanism and in both areas work needs to be done to change, one inside the individual and the other by addressing the social connections moving forward. For mine the copings relate to relationships, the addiction becomes the trusted relationship and when that fails then new relationships, or indeed aloneness (as an acceptance of the failings in having healthy relationships) are required or result. I like Maia Szalavitz’s take on addiction as learning. Anxiety is the core, the fear of others, of their judgement, in the individual with a low self esteem often resultant of psychological wounds inflicted in very early childhood. I work with Aboriginal men in Australia in a rehab and many of those have never known a way other than that which brings them to me and the often dysfunctional environment they go back to is the element I cannot do anything about and so often leads straight back to a very unhealthy coping ways they seek change from.
Thank you Terry. I think the discussion and all the educating that goes on here is just remarkable. As I read your posts and others -I get an array of light bulb moments that truly are just so wonderful to experience! This stuff just makes so much sense.
It is really nice Carl to see the enlightment that is broadcast here in these posts in an AOD world that is otherwise so full of archaic morally based ideas. This gives me hope when I read the notions which Mark and other contemporary authors and thinkers are presenting which, yes, do (re) light the bulbs of some who have had these ideas for some time but never been game enough to speak of them in what is also a highly judgemental environment
The idea of willpower comes out of an authoritarian, disciplinarian, punitive, paternalistic system of thought around human behaviour. The idea that punishment will make a person want to be “good”. What’s needed to break any bad habit, is the ability to see and weigh up different choices, using those front bits of the brain.
Matt we agree in dislike of the addiction and recovery words that not only medicalize but also stigmatize the problem
Rehabituate is interesting but isnt it incomplete to what the full benefits of the changes we make are ?
The limitations of language in capturing the ineffability and personal nature of experience. Everybody’s outcome, and purpose and “thing that fills the hole” that used to get filled by our addictive behavior…is going to be different. But maybe the process by which we get there could be done and described in a more salient, compassionate way, unlike the punitive, disciplinary nature a lot of treatment methods employ.
Sounds like you know this stuff Matt. Music to my ears. Beautifully written.
I’m reminded of Bad Science’s Ben Goldacre’s observation of many things in science: “It’s more complex than that.” I can’t think of any area of human inquiry where Ben’s perspective is more likely to be true than in neuroscience. Hooray for finding common ground upon which to begin building programs and applications that are useful, effective and reduce suffering.
Ben Goldacre also points out that bad practices in science are encouraged by the fact that so much money is riding on it – research grants, pharmaceutical companies’ profits, etc. etc..
Both your perspectives make good logical sense. Meaning that you both are on the same page help those who need it. in my years of counseling I have run into many factors that seem to be at the root of addiction. The main ones are emotions are not recognized and when they become out of control the person naturally gravitates to a substance to relieve those symptoms. Whether it is learned or biological is not the case but how we get people to begin recognize those emotions before they become so strong is the essence of helping them overcome the desire to use.
Marc, , it sounds like the dangerous, “absolute thinking” of the NIDA has been cracked to some extent.
The fact that the head of the NIDA is acknowledging that many one-time addicts get over it — for good — Is this major breakthrough.
One concern is that an official conclusion will be that those one-time addicts never “fully” had the disease of Addiction, or something.
In any event, your account of the debate has shown there was
mutual respect and understanding, great to hear.
Carlton-
I would like to hear some feedback on this issue also-“One concern is that an official conclusion will be that those one-time addicts never “fully” had the disease of Addiction, or something.” I have difficulty trying to account for this when folks approach me with it. Theres something there and I dont know how to explain it other than to say “its proposterous to think that way”. I wish someone on here would attempt to do a better job explaining it.
Tests for Malaria, Cholera, and other diseases, produce specific results.
But testing for Addiction is like testing a fan of a specific sport , or if a person loves Classical, Country, Punk, Speed metal music, and to what degree?
MRI and other scans will give indicators, but then what? How do you help, or “treat” a person for being a fan of something… or loving a certain type of music…and to what degree are they to be “treated” to?
I mean this rhetorically, to show that addiction is in a different category than a disease.
It certainly may LOOK like a disease, but as Bill said, when looked at more clearly, its something else.
Thanks Carlton! THAT’s very helpful!
I find that, when I am determined to find common ground with anyone, I’ll damn well find it.
Once I do, a bridge – however rickety – is built. Then the next step is to fortify it. Then that bridge becomes a place that feels safe enough to cross.
My sense is that you went into this conversation not only to express your own perspective with clarity, but also to hear hers… seeking that bridge.
I am so glad you did that, Marc.
Would MUCH prefer to build bridges… rather than walls.
We ARE evolving… even NIDA is evolving.
There simply are no absolutes when it comes to our understanding of the mind.
It is ever evolving.
As Mark Brady, another of my friends and teachers, quoted, above, ““It’s more complex than that.”
Progress!
Has anybody seen the bridge?
Where’s that confounded bridge?
GoodGod I love a metaphor.. and Led Zeppelin:
https://youtu.be/CWf5FYSK7Yc?t=3m12s
Marc-Thanks for humanizing Nora!
You helped me realize that she could be a possible advocate instead of this ogre against harm reduction she presents herself to be at times. This is good maybe.
What a wimp Marc!!! gee whiz ha ha
I forgive Nora– after all she is a medical doctor first and addiction fits the disease model pretty well until you look closely and see the flaws
I at first was of the ” of course its a disease” mentality when I first started looking at it with Smart Recovery and then slowly started to see it more clearly as you know .
So maybe there is hope yet– next up George Koob
I hear you, Bill. No time to reply specifically, but see below…. Indeed I am becoming a wimp.
You may be a wimp but you’re our wmp
and the best of the best wimps we know
WIMPS UNITED !!
Hi guys. I’m in the US right now, on Long Island. Gave a talk today, and our very own Carlton actually showed up — in the flesh. And then I sat on a panel of five “experts” — except that I was the least expert of the lot. Because I come to addiction as a scientist and they come to it as clinicians, social workers, helpers, treaters, people who save lives, or at least clear a path, as much as possible, for people on the front line to do the heavy lifting.
This was a meeting of a group called THRIVE, and the men on the panel represented other organizations who intervene on behalf of addicts and their families at the state or even national level. I’ll fill in the details in a subsequent post, with a link to a recording. Because I really admire what these people are doing. And their thinking, their talk, their way of conceptualizing addiction, and sure enough their use of the “disease” nomenclature is all dedicated to helping people in addiction get the services they need from a tight-fisted, profit-driven health care system, one of the worst in the developed world. They call addiction a disease because that’s how to get insurance companies and government programs like Medicaid to pay…and a big part of what they’re paying for involves MAT (medication assisted treatment — read methadone and Suboxone) which is basically saving lives more effectively than any other form of intervention currently used in response to the overdose epidemic.
When I listen to the horror stories and start to get a sense of the dedication and effort needed to fight back against a corrupt system, my philosophical disagreements with the disease label fade into the background. Much more so than when I look at the red and yellow splotches on Nora’s brain-scan slides. I still don’t think addiction is really a disease. But you could call it one — especially in the current life-and-death context of opioid addiction in the US — and that might be the best way forward in the dark lagoons of the American health-care system.
WTH! This has just seemed to come full circle Marc. The wheels have just come off the cart and it seems like we are back to where we started. This is just absolutely nuts.
Marc, what in important comment you make here. While it is of immense importance to challenge the stagnant concepts that underlie the study and treatment of addiction in this country, we must simultaneously–and sometimes separately–continue to work in the trenches with those fighting for their lives. These struggles are obviously related, but not one and the same. Calling addiction a disease is certainly more useful than considering addiction a bad choice, and has two obvious effects within our current healthcare system. The first is that it fits within the medical model and, as you point out, this readies it for insurance companies to address. On the other hand, it also opens addiction treatment up to becoming a profit driven industry which seems to edge out social and human concerns these days (at least in America). But, there does need to be both conversations happening simultaneously, one that propels us into a deeper more empowering understanding of addiction than that proposed by the disease model, and the other about what to do NOW with the system that is in place. Hopefully the former will continue to inform and influence the latter.
Hi Marc,
Note that a few hours earlier at your Port Jefferson presentation, the audience there in seemed accepting and hopeful to hear that addiction was something other than an life- long disease, and your presentation seemed quite clear about that.
I was not able to get to this second Panel discussion you are talking about here,
but since Insurance Companies will only offer financial support for the Disease Model of Addiction, perhaps there is some other “disease-like” reason for the current fatal epidemic of overdosing.
This is all true except for one major distinction that Maia Szalovitz makes. You can’t simultaneously destigmatize something, and also throw people in jail for it and expect things to change. There has to be a major paradigm shift, and it has to come from the people on the ground.… caregivers and the people with addictive disorders
Your point is well made and taken, but while it is a laudable goal to obtain help for people any way possible as a result of having to function within a corrupt system, as we know, finding aid is just the beginning of the journey. It is that process and the way we navigate it that is in many ways shaped by the words used to describe the condition. I always found it easier to stop than to stay stopped, a dreadful and damaging state of stasis that went on for far too long, and it wasnt until I started to really dig down and be exposed to the debates and literature and began to understand and internalize what you and others were trying valiantly to posit that I actually started to get past the shame and hopelessness and sense of impotence that the disease label and associated peer group practicioners had instilled in me. How perniciously deeply and thoroughly I had absorbed it and how it affected most aspects of my understanding of myself and my addiction without me even questioning it. I had to change that before I started making progress. The cause you have championed all this time is important. I would urge you to keep at it with vigour as a change in attitude seems to be taking place slowly but surely. Words matter.
It was good meeting you in Port Jefferson ,NY recently . Next time you run into Dr. Volkow be sure to tell her you were in Port Jefferson it is only 10 miles to
Shoreham, NY. where she lived.
BROOKHAVEN TOWN HONORS BROOKHAVEN LAB SCIENTIST
Upton, NY – Dr. Nora Volkow, Chair of the Medical Department and Director of Nuclear Medicine at the U.S. Department of Energy’s Brookhaven National Laboratory, is one of 13 women who will be honored on Tuesday, March 31, for their accomplishments and contributions to Brookhaven Town. The women will be the guests of honor at the Town-sponsored Women’s Recognition Night, as part of its observance of National Women’s History Month. Dr. Volkow will be recognized for her excellence in medicine.
A leader in drug abuse research, Dr. Volkow uses an imaging technique called positron emission tomography (PET) to view how addictive drugs, such as cocaine, affect the brain. In the 1980s, she discovered that the brains of heavy cocaine users frequently had regions where there is no blood flow, similar to stroke victims. Thus, Dr. Volkow is credited with being the first researcher to report that cocaine is toxic to the human brain.
Her recent research findings were reported in a Time magazine cover story on May 5, 1997. Dr. Volkow and her colleagues demonstrated for the first time in human subjects that cocaine causes euphoria by increasing dopamine, a chemical substance in the brain that is important in movement, motivation and reward. The researchers also found that cocaine users have a reduced glucose metabolism in the part of the brain known as the orbital frontal cortex, which is key to controlling and planning behavior.
“I am honored to receive this award from Brookhaven Town,” said Dr. Volkow. “Addiction is a devastating problem, and my hope is that my research will continue to contribute to greater understanding of the mechanisms underlying it. Brookhaven Lab is home to a regional center of drug abuse research, and using the state-of-the-art facilities available to me, investigating how drugs affect the brain will continue to be one of my research priorities.”
In related work, Dr. Volkow has also used PET in pioneering studies of the biochemical changes in the brain associated with alcoholism and aging.
After receiving her M.D. in 1980 from the National University of Mexico, Dr. Volkow completed her residency in psychiatry at New York University in 1984. During this period, she used Brookhaven Lab’s PET facility to study schizophrenia and to develop a PET radiotracer to measure cell growth in brain tumors.
At the University of Texas Medical School from 1984-87, Dr. Volkow led a research program using PET to investigate the toxic effects of cocaine. In 1987, she joined Brookhaven Lab to continue this research.
She became Associate Chief of Staff in the Lab’s Clinical Research Center in 1990 and was appointed Director of the Nuclear Medicine Program in 1994. Two years later, she was named Chair of the Laboratory’s Medical Department.
Dr. Volkow also has been an associate professor in the Department of Psychiatry at the State University of New York (SUNY) at Stony Brook since 1987, and, since 1994, she has been a lecturer in the Department of Psychiatry at Columbia University. She was recently appointed Associate Dean of the SUNY Stony Brook School of Medicine at Brookhaven Lab.
Brookhaven National Laboratory carries out basic and applied research in the physical, biomedical and environmental sciences and in selected energy technologies. Brookhaven Science Associates, a partnership between the Research Foundation of the State University of New York on behalf of SUNY Stony Brook, and Battelle Memorial Institute, operates the Laboratory under contract with the U.S. Department of Energy.
-30-
NOTE TO LOCAL EDITORS: Dr. Nora Volkow is a resident of Shoreham, NY.
Nora Volkov has always talked about “environmental factors, the importance of social support in recovery, diversity in outcomes”, you can listen to her prevention/ awareness campaign on the internet-youtube. Perhaps you were too much focused on your campaign against the disease model of addiction to notice…