Hi you guys!!!!! Okay, I give up. I was seriously considering ending the blog, at least for a while. It’s time consuming! Especially trying to reply to your thoughtful and heart-felt comments. (I know I don’t have to, but I usually just feel like it.) I have two courses to teach in the next four months, and then there’s that book that’s supposed to be completed by June. Although my publishers may be somewhat flexible, I do want to finish by June. It’s a hot topic now. It may not be so hot in a couple of years.
The fact is, I miss you. I miss my blog, which means I miss communicating with you, my readers. It feels like a chunk removed from my life. And although there are a lot of other things I can attend to, I have learned a tremendous amount from this blog. About addiction and treatment and recovery and suffering and courage and being human and hurting deep down and soothing that hurt…and finding other ways to soothe it, other ways to feel. I don’t want to lose that incomparable source of knowledge, wisdom, compassion…whatever it is. I continue to study, write, and give talks about addiction and recovery. I’d better keep learning what I can about how it works. But beyond that, I just want to stay in touch. Whether you’re a frequent commenter or a hovering spook, I’ve become attached. You’re a second family to me.
So…New Year’s Resolution: I’ll try to keep my posts shorter — each one doesn’t have to be an award-winning essay — and just send you tidbits of stuff that seem new and important to me and that you might appreciate learning about too. Since I seem to be a blogging addict, I can at least try some form of harm reduction.
So here’s the connection. Last week I went to Toronto to give a keynote talk at the annual conference of the Ontario Harm Reduction Distribution Program. What an eye-opener! I thought I knew something about harm reduction. That’s when nice people try to keep addicts alive and relatively healthy until they can quit, right? Not 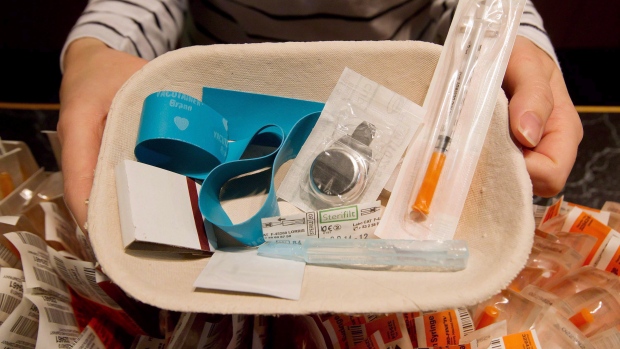 exactly. Here’s a cool radio piece about a harm reduction initiative in Amsterdam: supplying beer to serious alcoholics as partial payment for cleaning up the park they trashed the night before. Maybe this tells an important part of the story.
exactly. Here’s a cool radio piece about a harm reduction initiative in Amsterdam: supplying beer to serious alcoholics as partial payment for cleaning up the park they trashed the night before. Maybe this tells an important part of the story.
Well yes, harm reduction includes all that. But it’s also an entirely different approach to addiction, maybe you’d even call it a distinct philosophy. It doesn’t seem to have much to do with abstinence, for a start. Well, here’s how it came across to me. There were a couple of hundred people at this conference, and they make their living caring about people who most of society would prefer to write off. They seem to have unusually big hearts, and weird ideas to go with them. For example, teaching methamphetamine addicts to inject safely. How can you inject meth safely? The few times I shot meth, back in my chaotic twenties, I had no doubt that I was playing with death. One woman, a harm-reducer from London, Ontario, said, during her presentation: “We’ve distributed two million, one hundred and something thousand syringes this year. And we’re very proud of that.” Proud? I was shell-shocked. Proud? And when I passed the registration desk on day one, I was asked to try on the tourniquet. Arm-band, you mean, right? Isn’t it a nice navy blue color? And see how snugly it fits….velcro, you know.
I happened to be with my 25-year-old daughter that day. Still, as instructed, I pulled the thing around my upper arm, and sure enough those nearly-forgotten habits popped up to the surface of my consciousness, just as my veins popped up to the surface of my forearm. Besides being incredibly embarrassed in front of my daughter, who knows something of my history, I was simply grossed out. I haven’t shot drugs for over thirty years. Like is this some clever version of a registration tag, a door prize, or what? I couldn’t do it. Not that they were offering anything to go with it. But…it’s been too long. It was just yucck.
In keeping with my Resolution, I’ll end here. More on the conference, and some very interesting individuals I met there, next post.
Meanwhile, welcome back. And thanks for sticking around.
 Informed by unparalleled neuroscientific insight and written with his usual flare, Marc Lewis’s The Biology of Desire effectively refutes the medical view of addiction as a brain disease. A bracing and informative corrective to the muddle that now characterizes public and professional discourse on this topic.” —Gabor Maté, M.D., author of In The Realm of Hungry Ghosts: Close Encounters With Addiction
Informed by unparalleled neuroscientific insight and written with his usual flare, Marc Lewis’s The Biology of Desire effectively refutes the medical view of addiction as a brain disease. A bracing and informative corrective to the muddle that now characterizes public and professional discourse on this topic.” —Gabor Maté, M.D., author of In The Realm of Hungry Ghosts: Close Encounters With Addiction
Hi Marc,
Harm reduction.. Hmmm. My experience with this was exactly what you said.. I was taught by a nurse in a needle exchange centre how to inject safely and given as much of all the paraphernalia as I wanted!! Years later (no longer using anything and feeling very recovered) I found myself studying to work in case management with high risk teenagers in the housing sector, most had, at least, a drug problem. Anyway, during my study it became very very clear to me that the “harm reduction” was meant as a way of minimising harm to the community not the addict/user.
So, now I see those words, and I just think how ridiculous all those so called “caring” people are. They haven’t got a clue!! And I don’t believe they really want to know. Addiction is a messy topic, and as far as I can tell these “so called harm reduction” programs make the “powers that be” feel better but are if no real help to the suffering addict.
Just sharing my experience.. I hope someone else’s was a positive one.
Thanks,
Jo.
Hi Jo. Thanks for getting the dialogue going. A brief glance shows me that there is a hefty debate to be had.
I wouldn’t say they care only about the powers that be. But it’s true that controlling Hep C and AIDS is saving Ontario untold billions in health care. That part can’t be denied.
Where’s the middle ground? I don’t know yet.
Hi Marc,
I think either I haven’t communicated correctly or you may have misunderstood me re: powers that be, that’s not what I’m saying.. But they (whoever they are) at least in this country (Australia) certainly like to convince the addict and the general population that harm minimisation is all about minimising harm to the addict, when it most definitely is not. Sure, using clean needles etc will lower the risk of hep c and aids, etc… But, in the end, every addict I’ve ever known, including myself still took huge risks with paraphernalia, drugs, people and in their general way of living even after being shown how to reduce harm. Sure it has it’s place, but it’s a band aid, not the answer to addiction.
Cheers
Jo
I think I understood what you were saying perfectly. Like other respondents here, you question the value of HR for society relative to the addict him or herself. I was just focusing on health-care costs, which is part of the equation.
I think most respondents agree with you that HR is indeed a bandaid, and its value for the addict is certainly complex and debatable. But see Shaun’s comments below. He has another view.
I think harm reduction shows respect for a persons choice and opens a dialog on the subject that has mostly been taboo and shameful. I think that both the respect and open dialog creates dignity and awareness and clarity of a persons choice that they then can put into some perspective and make the choice to change through their own credibility rather than someone else’s coercion.
I like that view, Cheryl. There was one guy who got up and spoke, a trembling young man who looked pretty ill. Yes, he got it…AIDS I think. But he’s standing there at the mike, telling us what it’s like to be a gay Chinese man from a traditional family. It’s not good. And then he says: I’ve been clean since 2010. And everyone bursts into applause.
So, yes, he was helped (only a bit, I guess) to reach a place where he could quit. And his recovery was considered something both personal and heroic.
I have read the comments about freedom of choice;they are giving the addict the tools not the drug,so I still get to watch my stereo get stolen for the drug.I am 2yrs clean from alcohol and as long as no one is giving me a keg I am not out stealing to get the money to fill it.I`m not sure but I have heard everyone in Canada is covered with some type of health ins. Give them treatment not tools to continue an addiction.I would also think teaching people how to stay away from the needle would be better than how to use it right.I`m not saying anyone is wrong by posting that it gives the person the chance to choose when they want to quit using,we all have to find our way of dealing with our own addiction,do our own program. Thank you
I think you answered your own question, Paul. People need to find their own way, but the chance to do that might not come until later, possibly after some horrible disease makes it all the more difficult to do so. So HR does have value.
That’s not to say that people should be “forgiven” for crimes committed. I certainly would not go that far, and I think few others would either.
Marc,
I relate with your feelings… I feel depressed from reading about addiction and the sad stories. It is desperate for me. So I wanted to have a break and stop reading. Then I feel a big hole, because caring about addicts, addiction and recovery development has become part of my life. I guess I should do “harm-reduction” too.
But I don’t know how many % of addicts, if any, can do “harm-reduction” – most likely, they either “addicts” or “clean”. ?
Hi Jenny, You’d be surprised at the numbers that continue being addicts while depending on HR to stay alive. Until they quit. Or die. Or just keep going.
Yes, this blog almost seems like an obligation at times. We need to understand this stuff called addiction. SO MANY people are deeply affected.
Seems like that old-style methadone maintenance “treatment” is the ultimate form of what they now call “harm reduction”. I find it disturbing that it’s now considered sufficient treatment for heroin/opioid addicts in the US – so insurance/the state don’t have to pay for anything else on what is admitedly an uncertain path to abstinence and real recovery. So methodone addicts may be able to function better and hold a (fairly low-skill) job, are at less risk of OD, and don’t have to resort to crime to pay for their drug, but…. they are still addicts; they’re just addicted to something the state is willing to supply. People on methadone still abuse other drugs on top of it; many I know say kicking methadone takes longer and is more miserable than kicking heroin. I know several people personally who have also relapsed on buprenorphine treatment. “Harm reduction”, maybe. But seems like this reduces harm to society more than it reduces harm to the individual addict. Not that there’s necessarily anything wrong with that, but let’s not pretend it’s an adequate treatment for addiction.
P.S. Don’t quit yer blogging! Soon you will have another book to flog!
Hi Lisa
I think you have a misconception here. In the majority of cases opioid Substitution Therapy (OST) is not harm reduction, but rather treatment in and of itself. The individual who is stabalised on methadone or buprenorphine (suboxone/subatex) may still be dependent, but they are not addicted. Addiction does NOT equal dependence. Many are dependent on anti-depressants – they are not addicts.
You say:
“So methodone addicts may be able to function better and hold a (fairly low-skill) job, are at less risk of OD, and don’t have to resort to crime to pay for their drug”
Well that sounds pretty good to me! I would argue about the low-skill job scenario! Most who are correctly stabilised can perform any job.
The reason insurance companies are prepared to pay for OST is because it works – the data is unequivocal.
Having said that, OST is not a magic silver bullet. It is suitable for some and not for others.
Hi Shaun! See my reply to Lisa, below (I think). As shown, I agree that people can function quite well on methadone or bupe. I’ve seen it first hand. But then there’s the other bit….the boredom, living life in low gear. Taking a powerful drug every day of your life is going to narrow the range of experience, emotion, and possibility that’s available to you. Well maybe, as you say, that’s a pretty good deal for a lot of people. For others, it should only be a way-station.
The definitional issue, addiction vs. dependence, is too dicey for me this morning. But I will say that when people close to me are on antidepressants PERMANENTLY….it makes me sad.
Yup Marc
I was just trying to illustrate the point, but certainly many people are put onto anti-depressants as an end in itself, which is unfortunate and has consequences which are often not considered.
Buprenorphine seems to have less of a blunting effect from what I am hearing.
Have a good day. I’m off to see Jane Goodall lecture this afternoon, so that should be interesting.
Hi Lisa! Your views are similar to those of Jo, above. I kind of agree about methadone. It sure does save society a lot of grief, and it’s not much of a solution in the long run. I had a good friend who was on methadone for a few years after two decades of oxycontin. He functioned quite well, actually, as a professional. But methadone is BORING. Which is why he and quite a few others take up coke or crack as the icing on the cake. To paraphrase (forgive me, Leonard), that’s where the light gets in. Provides the day with some contour, some drama.
He jumped off his balcony and died a few years ago. After spending about half a million on crack. Not much of a solution.
But it’s a complex story, and methadone might be one of very few choices for some individuals.
Yes ma’am, blogging away again. And the first installment of that book is coming soon.
I have discussed the pros and cons of OST and the need for an effective middle ground here: http://addictioncapetown.blogspot.com/2013/05/opioid-substitution-therapy-treatment.html
I just started reading and saw methadone being discussed and that is so true. I use to be on methadone from 2008-2012 and after awhile when you develop a tolerance and that buzz wears off the person starts feeling drowsy, tired, and bored. I would up my dose but of course that did not give me that euphoric effect. I began shooting up heroin just for the rush and would then nod off ( I never used heroin to the point of passing out) so then I and my ex began smoking crack and that done after you feel the methadone coming on was a good blend and then to come down shoot up some dope or drink a few beers. Anyway, for almost a decade when I became involved w a guy that wasn’t an addict at the time but b/c he was the kind of guy that just wanted the easy way out in life, which led him to addiction I was exposed to this and became an addict myself. It began w/ alcohol (2005) and got to the point that w/out alcohol I had HORRID withdrawals and drinking at 6 or 7am, completely malnourished and even attempted suicide a few times b/c without it I felt horrid and with it I felt horrid but I just ended up in the psych ward. Then by 2007, out of the hospital and wanting to stay clean and sober I ended up tampering with opiates (mainly poppy pod tea and painkillers). By end of 2007 we were both hooked on heroin. It was to the point that I lied and stole from my own parents, constantly stealing money, valuables, and more money, it was sick. In 2008 I began methadone but still used since my then b/f was using. Then if I didn’t have dope I would drink and it was just a vicious cycle. For the next few years I struggled with this addiction and of course being with someone that too is an addict and those kind of people it just doesn’t work. And the thought of being alone was also terrifying b/c it just seems like there is nothing left. Then in 2012 I got off methadone and onto Suboxone and in mid 2012 I left the guy that introduced me to this lifestyle b/c now I had a job and was busy with that but after a couple weeks that depression and loneliness gets to you, you don’t know what to do with yourself but you don’t want to use but that’s all you can think of. Then one day by complete accident I met someone, someone that wasn’t a junkie or ex addict and was actually doing something with his life, I found out not only was he successful but he has made a big name for himself nationally and internationally. So of course finally being around someone sober and hardworking and very talented does have a positive impact but I still found myself depressed and drinking from time to time b/c of anxiety, which stemmed from not knowing which way to go to better myself and my life, since I wasn’t with just an average joe shmoe. 6months into our relationship I finally began school and one month later went on a binge for a week b/c of an emotional breakdown and not knowing what to do. After that I didn’t want to drink, crave, or get anxiety and depression and was so sick of slipping up every now and then. So, that guy would always ask “why do people even get addicted to drugs?” and I never even really knew the facts myself and then it hit me (and I was studying it in one of my classes). I should really start researching that and learn why. I was getting so sick of feeling unstable at times and now I was getting somewhere. Long story short, I began from the very beginning and learning what drugs mess with in the brain, which helped me better understand why I crave, get depressed, and have anxiety. I used to take antidepressants but that definitely didn’t help compared to the way I do it now. I’ve been clean from drugs an alcohol now and I NEVER crave, I’m only on Suboxone no other kinds of meds and all these years going from doctor to doctor to rehab to inpatient and out patient, AA and NA meetings, lordy lord and none of those worked! Learning what these drugs do and restoring that balance naturally by eating right, nutrition plays such a big role with my experience meaning getting nutrients that are needed for overall proper brain function (ex B6 helps in serotonin production as well as vit D3, and protein for the amino acids) also something I can’t live without are 5HTP and St. Johns Wort, which REALLY help with a positive mood, compared to prescription antidepressants which are crap, and of course EXERCISE. Another thing is surrounding yourself with positive, hardworking, and educated people and find a passion to devote yourself too, mine being is going to school to make something of myself. Working hard and feeding off these positive results and always trying to out do myself so I can hopefully be an MD of psychiatry one day. Addiction is so complex but yet so fascinating, and I NEVER thought that this would have been possible. Thinking my god am I ever going to be happy and feel positive. An addict has to learn to work for their happiness, finding a passion, and make that your new “drug” and getting in the habit of doing, which is something I have learned this past year from actually doing, and my god it works wonders. The people I used to be around were lazy and all talk but no do b/c that’s how they have been their whole life, fast and easy and that will lead to addiction b/c you do not want to actually work hard so instead of working and staying focused you just wanna hang out with friends after work and have some drinks and or do drugs. There is just so much that goes with addiction. Also for the past year I have been looking around trying to find a Dr out there that had gone through addiction and finally I have stumbled upon something so I can’t wait to actually read the book.
Omigod, Ania, that is hardly making a long story short. But thanks for sharing it with us. The happy ending is great to hear. And I guess the part that’s relevant to this week’s topic is that methadone just led you to further using, perhaps taking greater risks than before.
Good luck with your plans to become an MD. And meanwhile, maybe you’ve left us with the thought that finding the right man, and the right diet and exercise regime, beat harm reduction by a mile.
Hi Marc, I’m one of the many who are glad to hear from you again and glad you’ve decided to continue the blog. Love the harm reduction analogy! It makes sense to me, harm reduction does, as it’s realistic for one thing, and it can help to remove that “woe is me, I’m just a no-good-addict” mentality from people who are already acting self-destructively. The HR attitude in itself may help an addict feel (paradoxically) that, now that some of the rebelliousness in the behavior is removed or rendered moot, it may be time to give up the behavior altogether. Part of the HR philosophy, as I understand it, is not advocating the addictive behavior, but rather advocating sobriety as a worthy goal while helping the addict stay safe and as healthy as possible by removing some of the more harmful aspects of the addictive behavior. Anyway, thanks for raising the subject! Denise
Take it easy Marc. I don’t see that it is in anyones interest that you burn out, or shut down the blog either. Shorter posts and a willingness for the rest to engage with each other directly could work. No need to wait for Daddy to chime in to have a discussion of this kind.
With respect to harm reduction, there is a relevant meme that has emerged in the last week around the death by overdose of Phillip Seymour Hoffman. His death is no more or less meaningful than any other OD, but it provides a seed for dialog to crystallize around.
One of the commonest causes of accidental OD is the variable quality of street drugs, and it may well have been the key to PSH’s death. If harm reduction/medicalization were the working paradigm, he could have had a prescription for pharmaceutical grade heroin. By replacing street drugs with pure heroin of known potency, providing sterile needles and cutting the link to the self-destructive sub-culture that addicts now need to maintain their supply, PSH and many like him might still be with us with the prospect of controlling their use or quitting entirely in the future.
Does such a program amount to approving of addiction? I don’t see how. It is an acceptance that disapproving of the behavior provides is not a fruitful starting point for managing addiction at a policy level. Almost anyone who has seen the reality of addiction will tell you that it’s a trap and a most unlovely thing. But it isn’t about to go away and the law-enforcement approach has proven its worthlessness over the last 50 years. Harm reduction is of course a band-aid solution, but there is no prospect I can see of a silver bullet to “solve the problem
Hi Jeff. Great comment! It’s not so much Big Daddy as having learned as a child that it’s not polite to ignore people. Still, I definitely take your point.
I think your view on harm reduction is really sensible. My wife cried over Hoffman’s death, and I think we’re going to watch his movies this week and I’ll probably cry too. Preventing deaths like his and all the other negatives you mention is a powerful motive for sensible HR and medicalization. I hate to admit it, but calling addiction a disease might make it easier to “treat” in this way with zero implication that it’s a nice way to live.
Indeed, approval vs disapproval don’t seem to have any impact whatsoever.
By the way, did I mention that I watched — was riveted by — that documentary you sent me: The House I Live In. It was also screened in its entirety for participants at the pre-conference event last week.
Here’s a link for other readers: http://www.imdb.com/title/tt2125653/
Just watch it.
The documentary is an eye opener, the best of its kind. It is available on Netflix, or failing that it can be torrented from:
http://torrentz.eu/6ad4ddc2b6a6cb870e1927b134a26a7db36b8568
The material in the documentary is closely based on the path prepared by the HBO Series The Wire. This is a sixty episode (Five Season) drama, the creator of which is David Simon, who is featured in the documentary. The Wire is also best in class, a superb dramatic treatment of how the Drug war plays out between Cops and Dealers, Politicians, Labor Unions and Schools in Baltimore. Watch it and be enlightened.
Bravo Denise! I think you have captured the essence of HR.Harm Reduction is also an approach to prevention.I was a drug/alcohol educator and counselor and I used this approach in the classroom of the public high schools I went to.We tried to educate in a way that helps to keep our kids alive if they even if they experiment with drugs or alcohol.One thing I tried to teach them was the concept of synergism, when more than one drug/alcohol is used, in an effort to reduce overdoses.Most kids who experiment do not go on to have problems.But they need to survive these too often deadly years.This approach also gave me some much needed credibility with the young people.I was not presenting them with a “Don’t do this”message, which will fall on deaf ears anyway.And these are likely theears that need to hear this most.
I was also a counselor and a patient at a methadone program (MMTP).I was a counselor first sadly.My experience was that MMTP was helpful.It helped me and I saw that it was very helpful to many others.These are the unheard from addicts some of whom get clean and some who remain on methadone.Of those who stay on the methadone many have jobs and meaningful relationships and they find life rewarding.What could possibly be wrong with that?People who are against MMTP’s simply have not been in a position to evaluate it’s efficacy. I also took buprenorphine and it was very helpful.
I have been clean for years now but I spent the the great majority of my life on legal and illegal drugs.
I don’t know if I would go so far as to give a meth shooter a syringe but I would certainly give it to a heroin user if I couldn’t talk them into MMTP.So,if pressed,I guess I would.This is an example of one of the perils of HR;everybody has their own sense of what it is and how far it should go.
As an educator I drew the wrath of many schoolteachers for this approach.People get really bent out of shape when they hear many of the HR concepts, as we have seen here.This is probably the most problematic aspect of HR.One size does not fit all addicts/alcoholics despite the ease of this kind of thinking.I am all for AA/NA and have gone for years but I just know too many tales of doing it other ways that also have good endings.
Good luck with your work Marc.I enjoy the blog very much.
Hi Chris. You help us find balance in this debate. The fact that MMTP can often help people just doesn’t jibe with the lopsided degree of criticism you get from people outside the addiction community. I agree with you: they don’t get it.
The other point you make, which I think is critical, is the value of a HR approach for teens. Indeed, Just Say NO is not going to work. And kids this age just don’t have the judgement to consider the perils of their explorations. Keeping these kids alive and healthy is SO important. I doubt that they will find addiction to be fun and rewarding as a result of these lessons….so the only goal is to keep them safe until, as you say, most of them will move onward.
Hi Denise, This seems like a description of HR at its best. And I particularly like the point about rebelliousness no longer having any meaning. For some of us that could be very important. For me, the defiant/rebellious thing was a strong contributor to the overall pattern. I sometimes saw myself as a Robin Hood-like figure, scaling the castle walls to steal my treasures.
Hi Marc: I missed you too (and everyone else).
I remember spending years in that limbo, knowing I was screwed up, but unable to do anything about it. Probably ten years like that. No one could help me. I would fly into a rage if anyone tried. “What did they know about me???” You know, like that.
Thanks goodness I survived those years. There were a couple of close calls. Doesn’t harm reduction give people like that a chance to survive until the few of us who can get sober actually do?
That is quite a story about the tourniquet. I read somewhere that addiction is like a creased piece of paper. No matter how long the paper has been laid flat, once it’s folded over again, it folds to the same crease.
Peter
Hi Peter. Yes the “action memory” was right there, ready to be switched on. But so was revulsion. I guess, even in the old days, I would gross myself out shooting drugs and yet keep doing it. Maybe the build-up of that reaction eventually helped me stop.
You survived until you were ready — and that’s the point of HR for many people. It’s hard to argue with that…especially when you’ve been through it yourself.
Hi Marc I one of those former hovering lurkers stepping out of the shadow to comment as there seems to be some mischaracterization going on here of the role of harm reduction on the treatment spectrum. Here is a quote from Andrew Tatarsky’s Center For Optimal Living – that I think should clear up the confusion:
The stigma about people who use drugs in problematic ways but are not ready to stop is expressed in the criminalization of these people and the that most treatment programs will not treat them unless they commit to stopping. Most problematic users are conflicted and ambivalent about stopping or unclear about what they need to do. Effective treatments must engage them where they are in their ambivalence. This means accepting them in treatment before they are ready to commit to stopping. Then we can establish respectful, empathic, supportive, collaborative therapeutic relationships that enable comprehensive assessment and clarification of realistic goals and personalized plans for working toward positive change that suit each person. All positive change goals that are steps in the right direction are then seen as successes on the path toward one’s ideal outcome. This “harm reduction” approach extends the reach of treatment to the entire spectrum of problematic drug users rather than restricting treatment only to those people who are ready, willing and able to embrace abstinence at the beginning of the process. This shift in the focus of treatment makes treatment more attractive and appealing to a large number of people who are not “motivated for abstinence-only treatments.
Government statistics support [this position]. The annual household survey of drug use in America found that 40 percent of substance users who were determined to need treatment and want treatment did not get treatment because they did not want to stop. Most substance use treatment only offers abstinence as a goal and only accepts people in treatment who are ready to commit to stop. Problematic substance users who are using for many personal and social reasons that work in some way, such as self-medicating suffering, are frequently not able to embrace stopping as a goal until alternative solutions are available. Harm reduction theories accept active substance users so that the sources of suffering can be identified so that alternative solutions can be discovered. This will increase the users motivation to cut back or stop using substances.
This is a great argument, comprehensive and balanced. Indeed, it’s absurd to insist that people have moved beyond their ambivalence before help is available. Moreover, addictive drug use is amplified by trauma and anxiety. So anything that can help reduce the danger and uncertainty of “the life” is likely to move people along the spectrum toward controlled use and eventual abstinence.
Your statistic of 40% does not surprise me. Actually I was one of those. I sought help long before I was really ready to quit. In those days, HR was not in the dictionary. But I sought out therapists who could help me figure out what I was doing and find a way out. One psychologist refused to see me because I could not honestly say I was ready to quit. I still get pissed off when I think of that moralistic jerk.
P.S. Meeting people where they are seems like a core principle. And so does the importance of being realistic. That’s a lot of what’s missing from most treatment systems.
Marc, I’m so glad you’re going to continue blogging; there’s a conversation here that is unique … I always think of conversation as dialogue –> from the Greek “dia” + “logos” that translates into “a shared search for meaning.”
About harm reduction … It strikes me, in part, as a contradiction in terms; a person is still ingesting a substance that s/he is addicted to. I have no experience, either as a user or a carer, in this area … it makes sense medically (reducing likelihood of needle-borne disease, etc), but existentially? I wonder how many studies have been done (long-term) to show how helpful this approach is — how many people have ceased using, and have stayed off a drug.
I can only think of your experience with the tourniquet as a triggering one — as you wrote (in a sense), you were ‘right back there’. Another contradiction, it seems — a paradox — that to be in the presence of the tools of ingestion could only incite the urge to use. You, however, felt a “yuck” reaction, after all your years of walking away, walking away …
In the last few days, since actor Philip Seymour Hoffman died, I’ve wondered how you’ve thought and felt about his situation. One writer (link :http://bit.ly/1c44HfA) said of Philip’s end: “He was alone in his bathroom, compelled.” Those words break my heart, and speak to an elemental truth of addiction — “alone…compelled.” All the goodies, glories, and genius that a person can have … and his life ends there.
The only true harm reduction that I can imagine is the cessation of use … and the excavation of a soul. Your mention of “the unusually big hearts” of people in the HR field is a clue … the mention of “care” … and all I can think is that somehow we have to evolve into a form of self-care that does not include the use of whatever compels us to what addiction takes us to, eventually: fatal loneliness.
Jaliya, Good to see you back. But you HAVE had experience as a carer — for your brother. Not officially, of course, but that was certainly being a carer. I don’t think HR has to be defined so narrowly. There may be a profusion of ways we can help addicts stay safe until they’re ready to stop. The comments here have addressed many of these far better than I could myself.
Since you mention Hoffman, and since I know about your own personal loss, I can’t help thinking that loneliness itself may be a major part of the “harm” that stands to be reduced. That program in Amsterdam fostered fellowship and companionship among alcoholics, serious alcoholics, and that in itself seemed an important step.
That little flash of memory I experienced was far from anything capable of sending me back. Otherwise, I’d be living right on the edge, in which case almost anything could send me back.
Please look at some of these comments and see what you think.
Thanks, Marc … Yes, I’m reading and re-reading … trying to understand. I don’t yet see how harm can be reduced if use (addictive use) is not also reduced. It does seem a paradox to me … I see how the companionship amongst the folks in Amsterdam would lift a little of the devastating loneliness … but to continue to ingest the substance that does all the harm in the first place — would that not continue to damage one’s capacity to be in any kind of true relation (considering that in active addiction, one’s first and often only relation is with the substance)? I am ignorant of experience in the wider field — only know, really, what I have witnessed and experienced alongside people in my circle who have been addicted. I did work in the field for several years in the mid-1980s, in a program that was 12-step-based, and always sensed that *something* was not being addressed … and I do think that it was the unaddressed agonies of broken relation; the existential injuries (I keep thinking of your boarding school experience). ~ My brother…he couldn’t have met any success with reduced use, for he had lost all capacity for reduced use. ~ I do know one thing: that it will never work for us to consider addiction a ‘criminal activity’ — to dump more shame onto people who are in such pain only fuels the urge to use, to waylay consciousness and awareness …
See my next post!
I think good treatment for addiction is complicated. It may be that harm reduction is misinterpreted by certain institutions and providers. Then when you throw in commerce (what motive did that person have to put that band on your arm other than selling one?) the money to be made skews treatment.
But if the point of HR is to meet addicts where they are, and also work with them to continue to reduce to the point of abstinence, then it makes sense to me. This takes a level of sophistication that I think is lacking in the mental health field in a lot of areas.
We do something like this in SMART Recovery, the participant can choose not to be abstinent but they can keep coming without being shamed or coerced into stopping. We continue to teach what we know and they often stop as they learn about their addiction, share with others, get information and support…
I am glad you are back and not closing the blog! Occasional posts are way better than none. 🙂
Hi Suzy. Please see Mike’s comment above. Like him, you see the value of meeting addicts where they are. And so do I. And thank you for letting us know that this fits within the wider scope of SMART recovery. We have a lot to learn from you guys. And also, I think you’re right that the philosophy of harm reduction could be extended to other mental health problems….in ways that are sometimes hard to imagine. A professor of mine, Otto Weininger, helped to train us newbee clinicians to enter the world where the psychotic person lives, rather than try to convince him or her that this world wasn’t real.
Thanks for your encouragement. I will definitely keep at it for now!
Hi Marc
I am about to write and deliver a piece on non-abstinence based treatment, which I will send to you when done towards the end of next month. What is sad to me is that many people see harm reduction and treatment (as in abstinence based) as diametrically opposed, mutually exclusive ideologies. They are not. Rather, they exist along a continuum of care. The treatment modalities that I am seeking to develop embrace all points along this continuum and I am carrying the message that both are essential components of effective treatment and public policy.
As we know, the vast majority of people who meet the criteria for addictive disorders, or chaotic substance use, will spontaneously remit. Most drug use has a half-life. Many of these people may cause themselves great harm or even die during this chaotic period. Most never enter treatment because of the onerous requirements for abstinence. Harm reduction allows these people to stay alive and minimize the damage so they can go on to live productive lives. You can’t treat dead people! There is also no evidence that I am aware of to suggest that this prolongs substance use or results in more people using substances.
On the other end of the scale we have a small minority of substance users who have multiple and complex problems, including co-occurring psychiatric disorders, sub-optimal social conditions, massive issues of trauma and/or cognitive defects, all of which make combine to make their disorder seem like a chronic terminal disease (and in many cases it does result in diseases or acute conditions which cause death). For these people abstinence will (very possibly) never be an option. These individuals need to be treated with compassion, and certainly at times the treatment of such patients closely resembles palliative care.
Ultimately though we need to find balance and have no expectation to impose upon those we treat: neither the expectation of abstinence nor the presumption that abstinence is not possible. Our responsibility in the treatment of addictive disorders is to assist the individual in finding a place where they can make conscious decisions around their substance use. Harm reduction contributes to this process.
This is why we need to have these two options available in all treatment settings.
I have read about the Amsterdam project, and I think that it is worthwhile and meaningful, with a couple of provisos – Are they receiving any form of thiamine supplementation to prevent Wernicke-Korsakoff syndrome? Are they receiving assessment regarding their health/cognitive effects? Often a brief intervention along with the presentation of simple medical facts is enough to provide initial motivation to change using patterns. Personally I would like to see a scenario where they could receive the beer OR a food voucher of slightly larger value, so that although there is choice there is not the presumption that they will always take the beer. (thinking of Hart’s research!)
Good to see a new post. Please keep going because each post really challenges me to think carefully about vital questions and this leads to my growth.
Hello Dare Marc , Hello Dare S&S :
I have been walking into walls ( in a good way ) ever since Marc posted this . Deep in thought , I have asked myself 1000 times how to respond without getting into trouble .Yes that has happened . Harm Reduction in Blog posts if you will , my New Years resolution . I decided that preaching to the converted
( that’s You ) might be the way to go , the other way is far to exhausting .
I live in Vancouver B.C Canada and have seen the growth of and the Lives saved from a Harm Reduction perspective . Vancouver is home to the first Supervised Injection site in North America called Insite http://www.communityinsite.ca/ .
It also houses a Detox and treatment center Onsite , this combination is not reported often , as the Injection Site is far more salacious a issue . If you look at the website you will find that there have been a million injections ( yip , 1,000,000 ) and not one death in their more than 10 year existence . That’s success ! Supervised Injection site always made sense to me , outside of all the services offered and contact with health care professionals , referrals to everything from dentistry to housing to where to get free dog food for your pet .
The very pragmatics act of injecting yourself demands some supervision . Jebus forbid anyone on this blog has to go to the hospital or Doctor for treatment but if you do , just before your health care professional gives you the needle , simply ask ” Hey mind if I do that myself ? ”
Doesn’t matter if it’s a flu shot or anaesthesia before surgery , try it at the dentist . Then stand back and watch the “Ethics hit the Fan ” Some how drug addicts don’t deserve this information and must suffer infections and death on their own .
Harm reduction has been around forever just in different forms , mandatory seat belt laws , picture’s on cigarette packages , nutritional information on food packages , on and on and on . Have saved untold lives over the years , but once again some how “Drug Addicts and Drunks ” don’t qualify .
Love your articles
Good to see you back, Donnie. And thanks for the information and stats on what’s been happening in Vancouver. I knew about Insite….but not the rest. There does indeed seem to be a consensus emerging here, so you’re swimming with the current, bud. Drop me a line and let me know how you’re doing.
Hi Shaun. I love the “continuum of care” idea. In my next post you’ll see that I’m pretty sold on HR. But you say it quite eloquently: you can’t treat dead people. I am now starting to wonder where this idea came from, that HR and eventual abstinence are in any way opposed…. You ask the right questions. And from the little exposure I recently had at the conference, there seems to be general agreement that it’s the opposite. HR seems very capable of stabilizing people, and that’s a really important step.
Such an eloquent and inspiring post Shaun+Shelly, thank you.
HI Marc
Good idea…too much time spent and you burn out. I did same thing with my “think tank”.
LOL when I read about the Velcro shoot-up straps and the woman proudly proclaiming her needle giveaway count.
Now this a true story so you have to take my word for it. About 20 years ago I told my first wife that PC will be the biggest risk/threat to Western Society.It was just getting rolling in those days and we heard a lot of PC drivel from fellow parents when the girls were young. And some of the revisionist crap being taught was unbelievable. I am sure you will believe me when I say I was a major pain -in0-the-ass when I heard about misrepresentation of our history, science, social science, whatever
You are old enough to remember the day when Canadian schoolchildren were required to memorize “In Flander’s Fields” by John McCrae. Now they don’t. The poem, written by a Canadian surgeon (in ten minutes according to witnesses) became the most famous of WW1 a war replete with great poets.
Now an important part of Canadian history (and pride) has been swept under the rug as it involves OMG! war!!!!
Cheers and Welcome Back
JLK .
.
Hi John. You are funny and interesting as always (well usually). In Flander’s Fields the poppies grow…that’s all I remember.
I mostly agree with you about the PC invasion. Luckily it’s not that bad here in Holland. But I’m not even sure I understand what it is anymore. When I’m at the Sheraton in Boston and every f…ing server, desk clerk, porter, whatever they have at hotels, gives me a big beaming smile from the moment they lay eyes on me….is that PC? Is that what it is in America? We do not permit unpleasant feelings to register? Here in Europe, people are allowed to be snooty, grumpy, and just plain disinterested. I’ll take that.
What this has to do with harm reduction I haven’t got a clue. I guess you’re saying that we might as well call a spade a spade and do what we can to keep from being hit over the head with it.
Just for you JLK
http://nypost.com/2014/02/09/canadian-rehab-center-installs-crack-pipe-vending-machine/
Ok, so I’m back. This time to talk about meth injecting. Do not read any further if you are easily offended!
When it comes to sex, meth is a fantastic drug, especially when injected. It enables you to perform for hours with delayed orgasm. Yes, it can cause impotence, but viagra or caverject easily solves that problem! For this reason it is very popular amongst the men having sex with men (MSM) population.
On the down side, it lowers inhibitions and the use of condoms is reduced and needles are often shared. Because of the prolonged sexual activity lesions are far more common and blood borne viruses are easily transmitted. Hence HIV risk amongst injecting meth users is high.
So, teaching safe injecting is only part of the harm reduction strategy for this population. Along with this comes information on how to sterilize injections, the distributions of lube and condoms and general wellness services, along with HIV/STI/Hep testing and counseling. The UNODC United Nations Office On Drugs and Crime) has 9 deliverables to its harm reduction package for people who inject drugs (PWID), of which needles and syringe provision is only one.
The 10th component recommended by PEPFAR is outreach work. So, one aspect of harm reduction would be to use peer educators, many of whom who are current active users. To give you an example:
One of the organisations I have had dealings with employ an injecting meth user who goes out to MSM sex parties. He is a “top” (if you don’t know what that means ask a gay friend!) and he is a trained injector, which makes him a very desirable person to have at these parties. Before the sex starts he explains the risks involved, he prepares individual color-coded syringes for all the participants, ensures condoms and lube are available, checks and dresses any open wounds from previous injecting sites and discusses services available. When the speech is over he then injects each person in a clean and steralised site and the party begins! This guy has possibly saved more lives than most who are involved in abstinence based services and encouraged more people to seek appropriate interventions than any other outreach worker.
Harm reduction is pragmatism. These things are going to happen, like it or not! Evidence has shown that harm reduction significantly reduces the overall burden not only on the individual, but society at large.
To S & S
If that is your worst bring it on. Retired Commodity brokers are pretty thick so mild pejoratives such as above seem like normal exchange of ideas.,
While in my PERSONAL opinion it is complete and utter BS I am definitely not feeling put upon. .
One of my many hats is Economic Analysis as well as Geopolitical Econ. You combine that with alcoholism (recovered for 10 years) and I have a pretty good feel for what works and what doesn’t
But to make it short I just cannot understand the logic of giving an addict free tools of the trade and believe that is the road to recovery. As I well know addicts are the biggest liars around and they can tell the heart bleeders how helpful they are until the cows come home but it will be just the opposite in 90% of the cases.
The problem with the “war on drugs is demand. As long as people use drugs there will e someone to supply. Hardass rehab is the only way out for most..That means no drugs no hash pipes and needles, no methodone no nothing.
JLK.
JLK, I must respectfully disagree.
I don’t see those who use substances additively as “the biggest liars around” – certainly no more than many in big business. I see them as individuals who will do whatever it takes to protect what is sacred to them. Often that is drugs, like it is money for those who work on Wall Street. These are “normal” responses. The relationship with the substance is not purely chemical, but satisfies emotional needs that society as they have experienced it is unable to meet. Most of the people in our treatment setting do not lie, simply because of the non-confrontational therapeutic bond my therapists and health professionals establish with them.
This leads me to strongly disagree with the opinion that hardass rehab is the way out for most – I have personally found that hardass rehab can in fact cause a lot more harm than good in many cases. The fact is that most people who meet the criteria for addiction remit spontaneously – no rehab, no meetings. And in the case of alcohol many learn to drink in moderation.
Just because some people seem to benefit from such treatment approaches does not prove that they are effective treatment interventions. Many of those people would have spontaneously remitted or just needed time to reflect on their situation.
Sure, there are some who really do seem to struggle, but these people normally have co-occuring psychiatric disorders or sub-optimal social conditions. Some are just not ready for change, and for these harm reduction is essential.
As someone familiar with economic analysis you should also be aware of the cost of substance abuse and the related health issues. Harm reduction greatly reduces this burden on society as a whole, and even if one has no sympathy for the addicts, one should recognise that this pragmatic approach saves millions of public dollars.
In ten years of psychiatric home health serving the seriously mentally ill (schizophrenia, bipolar, major depression, PTSD) I found Harm Reduction worked much better than abstinence treatment. Harm Reduction can also be a path to abstinence.. There are many paths to recovery ! ! !
Thanks, Guy. Good to have your vote on this.
Marc, I wonder if it has ever struck you as odd that many of those who say, “addiction is a disease, etc.” are the same persons who oppose ‘harm reduction’ approaches
or label them as utterly misguided. If the effects of some actual disease can be curbed–e.g. gangrene in the extremities for diabetics– surely doctors and health professionals are obligated to undertake ‘harm reduction’ measures.
“Harm reduction” is generally opposed by those who say, “The addict makes immoral choices [like a bank robber]; there is no ‘cure’ unless he commits to stop making them.”
I want to clarify my opening sentence:
“I wonder if it has ever struck you as odd that many of those who say, “addiction is a disease, etc.” are the same persons who oppose ‘harm reduction’ approaches
or label them as utterly misguided.”
I meant, *those nonmedical persons who say….* I am NOT speaking of medical persons, psychiatrists, neuroscientists; I am speaking the spokespersons for abstinence-based groups and 12-Step approaches. These encourage members to think and say, “I have a disease.”
Hi NN
I consider addiction a disorder not a disease and as most who follow this post know I am a member of AA ( we NEVER call it “12 Step”…only outsiders from what I have heard in the last 10 years)
I believe the founders of AA; Bob and Bill, made the correct decision to refer to alcoholism as a “disease”. Their reasoning was not medical but psychological. In those days (1930’s) alcoholics were considered to be morally broken. By calling it a disease it helps the victim to skirt the moral issue and recover self respect. And you MUST know that without self respect you cannot recover from addiction. Besides my Dr and I decided that argument was tantamount to angels and pinheads.(Figure of speech)
JLK
JLK
I must admit I’m even more confused. I think you’re saying that the moralists oppose HR while the disease-ists don’t — not should they — given that this approach corresponds quite closely with the standard medical approach to disease.
If that’s what you’re saying, I get it….. And it may justify one or two cheers for the addiction-is-a-disease camp.
Great blog, Marc.
Please don’t go away, blogs don’t need to be long. In fact, many say they should be short.
Mind you, your short blog has resulted in many comments and LOTS of work for you.
Still, please don’t go away, even if you can’t respond to all the comments. We’d understand.
Thanks, David. But YIKES it’s true, so many comments triggered by those few words. And I’m trying to tell myself I really don’t have to respond, at least not in any length…..but so far my treatment is far from complete.
I’ve also heard that shorter posts are more effective. And if this is an example, it’s probably true. Now I need to be my own student and give myself STRICT word limits. Hopefully I’ll get there….
PS. I have a new website at http://www.sharingculture.info focusing on historical trauma. Only the first stage of development, more of a ‘marketing’ tool at moment. Feedback appreciated. Best wishes for 2014 to you, David
I took a quick look at your site. Man, you’ve been around the block. I didn’t know you were connected to Wired In….
You probably know that your message seems to intersect with that of Bruce Alexander when it comes to the relation between alienation and addiction.. Gabor Mate is going there too. I’d like to post a link to your site, so please feel free to give me a nudge if I write anything related to cultural disruption/domination….and I can insert the link right there.
Yes, I was Wired In. Started it as WIRED in late 1990s, changed its name and was developing initiative ever since. Ran Daily Dose and developed the web community Wired In To Recovery. Trouble is I could never get funding.
Bruce Alexander’s writings inspired me and Gabor is brilliant. Any publicity for Sharing Culture will be great, thanx.
I agree with so much on here. Please dont stop blogging even if it is four sentences – they are four sentences that allow other people to talk and discuss and find that community which half the time they disagree half the time they may agree but it is a space for discussion about this that is unique and lacks prejudice of any sort.
I understand where you are coming from on this, i found myself well again and somehow in a job that has demanded so much that I have also stopped writing and this post has given me the impetus to start again.
Harm reduction is a huge topic in my head – and when I have time I will respond properly.
This is very nicely put, Shaun,
As we know, the vast majority of people who meet the criteria for addictive disorders, or chaotic substance use, will spontaneously remit. Most drug use has a half-life. Many of these people may cause themselves great harm or even die during this chaotic period. Most never enter treatment because of the onerous requirements for abstinence. Harm reduction allows these people to stay alive and minimize the damage so they can go on to live productive lives. You can’t treat dead people! There is also no evidence that I am aware of to suggest that this prolongs substance use or results in more people using substances.
On the other end of the scale we have a small minority of substance users who have multiple and complex problems, including co-occurring psychiatric disorders, sub-optimal social conditions, massive issues of trauma and/or cognitive defects, all of which make combine to make their disorder seem like a chronic terminal disease (and in many cases it does result in diseases or acute conditions which cause death). For these people abstinence will (very possibly) never be an option. These individuals need to be treated with compassion, and certainly at times the treatment of such patients closely resembles palliative care.
That phrase is very apt, I think:
“combine to make their disorder seem like a chronic terminal disease.”
What seems to happen in some treatment and self-help groups is that *everyone* is told that. To scare the hell out of them. Depending on who’s in the group (proportion of remitting vs. hopeless ‘terminal’ patients), a minority, perhaps substantial (30%), will after a year or two, be in some sort of recovery.
These people will then say, “Program X saved me from certain death, from this terminal disease.” Program X is not be congenial to many of the complex, terminal cases (the small minority) you describe; they will quit and some will die. Those in Program X will say, “They did not work the program, so that’s what happens.”
Exactly! In fact, just by choosing to enter treatment many people are on the way to recovery. you could ask them to do pushups or recite nursery rhymes and this group would show improvements! Add to this a good therapeutic relationship, and no matter the therapy, the person stands a good chance of recovery.
Those on the other end of the scale need something far more specialised, and are often not given it because they are seen to be “not working the program”!
“Compassionate Healing.” “Harm Reduction” sounds like engineers containing a nuclear spill. (Addiction can feel that way, I know.) But “Compassionate Healing” is how I like to say it. And I believe in it, too. For all of us.
My husband and I began a harm reduction program last year to reduce our drinking. By Christmas we were alcohol free 4 days a week and drinking 3 days. As many of you pointed out, abstaining for a period to reduce harm is really about waiting for your next drink/whatever. My whole attitude to drinking changed over that time. I had become fully cognisant of the fact that my drinking was driven by addiction. It took the joy out of it (is that a good thing or a bad thing?). We travelled for 3 weeks with our kids over Christmas so abstinence went out the window (we had a great time in the snow in Finland). We’ve come home to a drought on our property … devastating conditions for our stock. Abstinence is still out the window as we struggle emotionally with not being able to change the weather but desperately need to. Its only a matter of time before cognitive dissonance and my future self will speak up and we will start all over again but in the meantime … I’m back to enjoying my daily indulgence (I’m sure that is bad!). Sigh. The merry-go-round of addiction continues.
Talking of harm reduction: Crack Pipe Vending in Vancouver http://www.ctvnews.ca/canada/vancouver-home-to-canada-s-first-crackpipe-vending-machines-1.1677066#ixzz2spaXdqtr
I am a believer in harm reduction and the spread of diseases associated with drug use and unsafe sex.
This I think is covered through the initiated government sponsored programs that give out free supplies to active participants of this risky activity, like condoms, needles and pipes.
Although this program reduces harm in the in-term, by helping minimize the spread of diseases. It does nothing in helping people and only condones and enables users to continue that use.
I believe we must step up our efforts in helping others free themselves from addictions.
This holds true with a supervised injection site here in Ottawa, which is only a band-aid approach, a half hearted effort in saving lives and does nothing in treating the underline issues and helping the addict overcome his addiction.
When a person who becomes addicted to any mind altering substances their choices have been consumed by that drug, and can no longer make healthy decisions.
This is where we must step up our efforts and take that right for choice away from that addict who is making those unhealthy choices and is affected by the negative consequences of their use.
We must stop enabling and start fighting back, by implementing a harm reduction strategy and or mandatory detox and rehabilitation which will address all the underline issues of that person who suffers.
No one should have to suffer; all addicts deserve the chance to have a good life free from the bondage of drugs. Some however need a harm reduction approach to realize that dream? We have a “means to an end” through the methadone and suboxone program, for those who suffer from the addiction to opiates.
I believe addictions should be covered under the ministry of health and not the criminal justice system. If a person is suffering from a mental health issue they can be admitted to a Mental Health hospital to get the help they need.
I believe those who suffer substance abuse, also suffer mental illness, due to the fact that the drug has altered their brains in such a way that they can no longer make healthy decisions under the influence.
There was a time in my life when I suffered from the addiction to intervenes use, from cocaine, to opiates and prescription drug.
If there was a program available at that time that would have taken my right for choice away from me and committed me to a facility that would have helped me, It might have saved my marriage, my job, my life that I once new, free from substance abuse.
Instead I suffered for many years; luckily I avoided the curse of Aids and other diseases, but lost everything else that meant anything to me.
This is why I must stand up against a supervised injection site facility that supports the continued use of intervenes drugs, and offers no solutions but only adds to the problems…
Hey very nice website!! Guy .. Excellent .. Superb .. I’ll bookmark your website and take the feeds also?KI’m happy to find numerous helpful information right here within the publish, we’d like work out extra strategies on this regard, thanks for sharing.
I am 5yrs clean from alcohol and in Australia. please Give them treatment not tools to continue an addiction.I would also think teaching people how to stay away from the needle would be better than how to use it right.I`m not saying anyone is wrong by posting that it gives the person the chance to choose when they want to quit using,we all have to find our way of dealing with our own addiction,do our own program. Thank you
Hi Meshack. I’m afraid you won’t get replies here as this post is very old — roughly three years old. Please catch up with us on more current posts. Your views, even if they are not shared by all, are certainly welcome here.
And by the way I agree that getting people off the needle is by far the best option!