
I seem to have become a movie critic. A month ago I posted on Ben is Back and yesterday I watched A Beautiful Boy on a flight home from San Francisco. And what I get at the end of each movie is a big fat nothing. There is no conclusion, no understanding, no ground from which to move forward.
 With Ben is Back, there was Julia Roberts’ compelling angst, and now, with A Beautiful Boy (which I also read), we feel that intense heartbreak of a parent who can do nothing more to help.
With Ben is Back, there was Julia Roberts’ compelling angst, and now, with A Beautiful Boy (which I also read), we feel that intense heartbreak of a parent who can do nothing more to help.  Only to keep loving…and losing…as if his son had cancer or leprosy. I guess I’m mad and that’s why my words are coming out this way. There is something fundamentally wrong in these portrayals. Yes, they get the drama, the heartbreak, the power of drug highs. They get the agonizing schism between the teen or young adult lost in drugs and the (generally divorced) parents who still love their kid intensely. All that is worthwhile and important. But what they don’t get is the experience. They don’t even try to approximate, to estimate, to guess at what these young drug addicts are experiencing (other than deep sighs and stretches and rapturous smiles). Why is this so opaque?
Only to keep loving…and losing…as if his son had cancer or leprosy. I guess I’m mad and that’s why my words are coming out this way. There is something fundamentally wrong in these portrayals. Yes, they get the drama, the heartbreak, the power of drug highs. They get the agonizing schism between the teen or young adult lost in drugs and the (generally divorced) parents who still love their kid intensely. All that is worthwhile and important. But what they don’t get is the experience. They don’t even try to approximate, to estimate, to guess at what these young drug addicts are experiencing (other than deep sighs and stretches and rapturous smiles). Why is this so opaque?
 I mean, if we can create film after film about the Vietnam War and experience the shame, guilt, and horror of soldiers watching their friends die and their deepest values twisted inside out, why can’t we even come close to portraying — not what the parent is feeling — yes, that’s important too — but what the young addict is experiencing? What could be more dramatic than that? (And isn’t that supposed to be the crisis of our time?)
I mean, if we can create film after film about the Vietnam War and experience the shame, guilt, and horror of soldiers watching their friends die and their deepest values twisted inside out, why can’t we even come close to portraying — not what the parent is feeling — yes, that’s important too — but what the young addict is experiencing? What could be more dramatic than that? (And isn’t that supposed to be the crisis of our time?)
 With Ben and Nic, there are plenty of scenes that broadcast, almost prostitute, the sense of shame that these young men feel about their addictions and the deep hurt they cause their parents and siblings. Okay…shame. We get that addiction confers shame, which makes it harder to stop and harder to connect. But there’s so much more that’s missing. What is it that gets these kids to go back to their dealers and using buddies and half-empty girlfriends to do it again? To throw it all away, even after a year or more of “sobriety?”
With Ben and Nic, there are plenty of scenes that broadcast, almost prostitute, the sense of shame that these young men feel about their addictions and the deep hurt they cause their parents and siblings. Okay…shame. We get that addiction confers shame, which makes it harder to stop and harder to connect. But there’s so much more that’s missing. What is it that gets these kids to go back to their dealers and using buddies and half-empty girlfriends to do it again? To throw it all away, even after a year or more of “sobriety?”
In an online interview, Nic Sheff, the “boy” on whose story the book and movie are based, describes meth as providing “the feeling I’d been looking for my whole life.” We hear that a lot in stories of hard drug use (heroin and meth), and these movies actually provide skittery sci-fi sounds suggesting that the drugs are broadcasting an irresistible homing signal. But that’s way too easy. Rather than imagine that this was our singular goal since first grade, we need to look at the cluster of feelings that we have been trying to get away from.
 This word “sobriety” might be a way in. What feels so miserable about sobriety (the kind that’s required rather than chosen)? I can tell you, in case you’ve never been there. It’s the boredom, the emptiness, the contrivance, the feeling of being who you’re supposed to be…which requires leaving behind the compelling drive to explore your own identity, choices, and consciousness. Who in Hollywood tries to portray that? The intensely creative moment of throwing out the norms and choosing, at the risk of one’s own existence, to reach for moments of awareness defined completely on one’s own terms.
This word “sobriety” might be a way in. What feels so miserable about sobriety (the kind that’s required rather than chosen)? I can tell you, in case you’ve never been there. It’s the boredom, the emptiness, the contrivance, the feeling of being who you’re supposed to be…which requires leaving behind the compelling drive to explore your own identity, choices, and consciousness. Who in Hollywood tries to portray that? The intensely creative moment of throwing out the norms and choosing, at the risk of one’s own existence, to reach for moments of awareness defined completely on one’s own terms.
There’s nothing moral or immoral about it. Taking powerful drugs can be a creative act, often with dire consequences. It’s not about the skittering sci-fi sounds of what is supposedly happening to your brain. Or the kiss of thanatos that inspired Freud and the Velvet Underground both. It’s the reach…for something so very different…from the monotony of living in our TV-tailored culture and obeying the commandments of family and love without ever having created  either one. Yes, we want that. But at 18 or 20, we can’t create it. We can only rent that property from parents who settled there and established a home there. We can only copy, and please, and behave ourselves, trading our youthful energy for the security we could never find elsewhere. And guess what: that’s not enough.
either one. Yes, we want that. But at 18 or 20, we can’t create it. We can only rent that property from parents who settled there and established a home there. We can only copy, and please, and behave ourselves, trading our youthful energy for the security we could never find elsewhere. And guess what: that’s not enough.
So we find our own kind of creativity and culture: the powerful technology of present-day drugs and the immensely attractive inclusion of like-minded venturers…and that moment of going back to being entirely unbound…that’s what we seek, and often find. And sometimes that’s what destroys us…and perhaps our families too. It just disappoints me hugely that all the power and skill of Hollywood has not even ventured there, not even peered under that rock…at least not lately…in the black-and-white disease-minded culture of “you’re either one of us or you’re some unfortunate mutant.” What the fuck? We can do better than that.
(I’m aware, in re-reading this, that it’s only one slant. My target here is the middle-class confusion and emptiness that often promotes drug experimentation in teens. That’s the setting in both films. Intense socioeconomic hardships can also propel drug use, as can trauma, loss, depression, and other challenges. And yes, drugs can be addictive — which is a causal force in itself. These other drivers of addiction are discussed in many other posts by me and my guest contributors.)

 Ben seems to be trying with great determination to keep away from drugs. Yet the demon of addiction is doing pushups in the parking lot, just as they warn at the 12-step meeting he attends with his mom. He finds a bag of dope in the attic, but manages to avoid taking it and gives it to his mother instead. He looks the other way when dealers and drug buddies from his former life show up magically on elevators and at car windows.
Ben seems to be trying with great determination to keep away from drugs. Yet the demon of addiction is doing pushups in the parking lot, just as they warn at the 12-step meeting he attends with his mom. He finds a bag of dope in the attic, but manages to avoid taking it and gives it to his mother instead. He looks the other way when dealers and drug buddies from his former life show up magically on elevators and at car windows.  He bravely endures the cultural ambiguity of an American Christmas and tries his best to connect with his sibs and step-sibs. He’s a good guy, and he fights the good fight, but…well I don’t want to spoil it in case you decide to watch it.
He bravely endures the cultural ambiguity of an American Christmas and tries his best to connect with his sibs and step-sibs. He’s a good guy, and he fights the good fight, but…well I don’t want to spoil it in case you decide to watch it. Instead, the usual “Reader’s Digest” simplifications are offered. For example, Mom meets the doctor who first prescribed pain pills, which got Ben “hooked” years ago, and says she hopes he dies a horrible death. We know that the OxyContin surge in the 80’s and 90’s did increase exposure to opiates and fueled increased rates of addiction. But to continue to blame doctors is insane. As
Instead, the usual “Reader’s Digest” simplifications are offered. For example, Mom meets the doctor who first prescribed pain pills, which got Ben “hooked” years ago, and says she hopes he dies a horrible death. We know that the OxyContin surge in the 80’s and 90’s did increase exposure to opiates and fueled increased rates of addiction. But to continue to blame doctors is insane. As  The 12-step presence is portrayed somewhat accurately. Both the good (fellowship, honesty, and mutual respect) and the not-so-good (brain washing, propaganda, and the all-or-none trappings of the disease model) correspond well enough with reality.
The 12-step presence is portrayed somewhat accurately. Both the good (fellowship, honesty, and mutual respect) and the not-so-good (brain washing, propaganda, and the all-or-none trappings of the disease model) correspond well enough with reality. There is some recognition that addicts have choices. Ben fights his impulses bravely, and he makes sensible choices to avoid contact with the people and places that serve as triggers. And yet there is this creepy sense of fatalism sneaking up on Ben and other addicts. As though whatever choices they think they’re making, they’re bound to succumb. By the way, addiction isn’t referred to as “a disease” in this movie. Yet the miasma of an alien presence or infection lurks behind much of the dialogue and plot.
There is some recognition that addicts have choices. Ben fights his impulses bravely, and he makes sensible choices to avoid contact with the people and places that serve as triggers. And yet there is this creepy sense of fatalism sneaking up on Ben and other addicts. As though whatever choices they think they’re making, they’re bound to succumb. By the way, addiction isn’t referred to as “a disease” in this movie. Yet the miasma of an alien presence or infection lurks behind much of the dialogue and plot. Junkies are portrayed as zombies. They are the opposite of clean. They’re dirty. They hover in alleyways, under bridges, around trashcans brimming with burning litter. It’s a classic and grossly overdone stereotype. When I was shooting heroin or morphine in my twenties , garbage-strewn alleys and river banks were not my preferred home away from home.
Junkies are portrayed as zombies. They are the opposite of clean. They’re dirty. They hover in alleyways, under bridges, around trashcans brimming with burning litter. It’s a classic and grossly overdone stereotype. When I was shooting heroin or morphine in my twenties , garbage-strewn alleys and river banks were not my preferred home away from home. But here’s my biggest beef. People who take drugs are shown to be occupied by some demonic force (or disease, or what have you) that makes them another species. They are not anything like normal people. They live in a different world, they’re not to be trusted, and they ought to be sent away to residential rehabs (where they won’t infect the rest of us) until the demon is exorcised — itself a rare event. This dichotomous “us vs them” perspective is the real message of the movie.
But here’s my biggest beef. People who take drugs are shown to be occupied by some demonic force (or disease, or what have you) that makes them another species. They are not anything like normal people. They live in a different world, they’re not to be trusted, and they ought to be sent away to residential rehabs (where they won’t infect the rest of us) until the demon is exorcised — itself a rare event. This dichotomous “us vs them” perspective is the real message of the movie. balance to their lives — what I referred to as “substance” last post. The cause of addiction can be found in mall culture itself (portrayed in the movie as a sort of heaven on earth), the rampant commercialism that sucks meaning out of day-to-day life, the often immutable stamp of privilege vs. poverty and the stultifying dead-end lives of those who don’t make the cut. Not to mention the sheer hypocrisy of a society that proclaims Christian values but rewards self-serving, self-protective priorities. I wonder if Ben was infected by these horrors rather than a magical drug high, and whether that’s what made it so hard for him to quit.
balance to their lives — what I referred to as “substance” last post. The cause of addiction can be found in mall culture itself (portrayed in the movie as a sort of heaven on earth), the rampant commercialism that sucks meaning out of day-to-day life, the often immutable stamp of privilege vs. poverty and the stultifying dead-end lives of those who don’t make the cut. Not to mention the sheer hypocrisy of a society that proclaims Christian values but rewards self-serving, self-protective priorities. I wonder if Ben was infected by these horrors rather than a magical drug high, and whether that’s what made it so hard for him to quit.
 A substance is what fills up a space. The lack of substance equals, well, nothingness. When people talk about their addiction they often talk about a sense of profound emptiness, a psychological void, that gets filled by a something they can only get from what they’re addicted to. To replace a sense of nothingness with a sense of somethingness (what else to call it!) is more powerful than words like “pleasure,” “relief,” or “satisfaction” can possibly convey.
A substance is what fills up a space. The lack of substance equals, well, nothingness. When people talk about their addiction they often talk about a sense of profound emptiness, a psychological void, that gets filled by a something they can only get from what they’re addicted to. To replace a sense of nothingness with a sense of somethingness (what else to call it!) is more powerful than words like “pleasure,” “relief,” or “satisfaction” can possibly convey. Berridge has compared this urge to the desperation of a starving animal seeking food. So it may be useful to view substance and behavioural addictions as fulfilling biological needs, or at least their psychological
Berridge has compared this urge to the desperation of a starving animal seeking food. So it may be useful to view substance and behavioural addictions as fulfilling biological needs, or at least their psychological  expression. Whether we take pills, snort powder, smoke, or inject, we are putting something into our bodies. This “inputting” is a behavioural prototype. It’s primal. It’s how we eat. In the case of binge eating, the target of the behaviour makes obvious biological sense. But perhaps all behavioural addictions relate to biological needs: e.g., winning against competitors (gambling), sexual needs (obviously sex and porn addiction), even social inclusion
expression. Whether we take pills, snort powder, smoke, or inject, we are putting something into our bodies. This “inputting” is a behavioural prototype. It’s primal. It’s how we eat. In the case of binge eating, the target of the behaviour makes obvious biological sense. But perhaps all behavioural addictions relate to biological needs: e.g., winning against competitors (gambling), sexual needs (obviously sex and porn addiction), even social inclusion  (internet addiction) and resource acquisition (compulsive shopping). In my book, The Biology of Desire, I make the case that addiction serves symbolic goals. For example, the warm feeling you get from opiates symbolizes the warmth that comes from being hugged or cuddled (no small matter for us mammals).
(internet addiction) and resource acquisition (compulsive shopping). In my book, The Biology of Desire, I make the case that addiction serves symbolic goals. For example, the warm feeling you get from opiates symbolizes the warmth that comes from being hugged or cuddled (no small matter for us mammals). of addicts in downtown Vancouver, mostly aboriginal, mostly from foster homes, mostly abused or neglected in childhood, highlights the enormous holes in the lives of people with devastated attachment histories — holes filled by drug use.
of addicts in downtown Vancouver, mostly aboriginal, mostly from foster homes, mostly abused or neglected in childhood, highlights the enormous holes in the lives of people with devastated attachment histories — holes filled by drug use. 

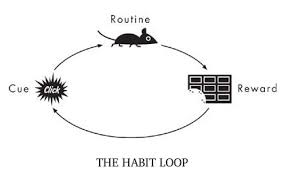 even as the desires and expectancies continue to strengthen. Is that pathological? No more than being in love with a hurtful partner, or praying to an unresponsive god, or being devoted to a sports team despite their string of losses. When the power of a reward arises from strong emotions and needs, the tendency to pursue it isn’t rational. When we seek and find that thing again and again, then, through learning,
even as the desires and expectancies continue to strengthen. Is that pathological? No more than being in love with a hurtful partner, or praying to an unresponsive god, or being devoted to a sports team despite their string of losses. When the power of a reward arises from strong emotions and needs, the tendency to pursue it isn’t rational. When we seek and find that thing again and again, then, through learning,  the synapses of our brain form into dense networks (pathways of connected neurons) that become very difficult to circumvent. Learning on overdrive, through repetitive need-satisfaction, is habit formation — addiction is a deep and insidious habit.
the synapses of our brain form into dense networks (pathways of connected neurons) that become very difficult to circumvent. Learning on overdrive, through repetitive need-satisfaction, is habit formation — addiction is a deep and insidious habit. expectancies and emotions become attached to a specific goal, leading to behaviours that are partly automatic — and partly not. Habit formation results in automaticity, sensitization to some rewards, and desensitization to others. The brain changes seen in addiction are just the biological underpinnings of this natural learning progression. And…they can continue to update; they’re not carved in stone.
expectancies and emotions become attached to a specific goal, leading to behaviours that are partly automatic — and partly not. Habit formation results in automaticity, sensitization to some rewards, and desensitization to others. The brain changes seen in addiction are just the biological underpinnings of this natural learning progression. And…they can continue to update; they’re not carved in stone. But what blows me away conceptually is how this narrowing of the available, reachable, usable social environment precisely parallels the narrowing going on in one’s brain. My synapses fell in line, in pathways and networks that had a single purpose, so to speak, rather than multiple pathways supporting
But what blows me away conceptually is how this narrowing of the available, reachable, usable social environment precisely parallels the narrowing going on in one’s brain. My synapses fell in line, in pathways and networks that had a single purpose, so to speak, rather than multiple pathways supporting  multiple purposes. This “narrowing” in the brain corresponded with a shrinking or narrowing in my available environment. Neither is pathological. Both, especially both together, create a kind of prison.
multiple purposes. This “narrowing” in the brain corresponded with a shrinking or narrowing in my available environment. Neither is pathological. Both, especially both together, create a kind of prison.

 the proliferation of gun ownership in the US and the political voices that advocate it. I guess you could say it’s an emotional topic for both of us. But we differed on a sort of thought experiment: What would it be like if people could make guns on a 3D printer and those guns were entirely untraceable? Would that be a bad thing because there’d be more guns around (her point) or a good thing because the NRA and its right-wing supporters would lose their influence (my point)? The content of the argument hardly matters. Neither of us had ever thought about plastic guns before. We were speculating, and then discussing, and then debating.
the proliferation of gun ownership in the US and the political voices that advocate it. I guess you could say it’s an emotional topic for both of us. But we differed on a sort of thought experiment: What would it be like if people could make guns on a 3D printer and those guns were entirely untraceable? Would that be a bad thing because there’d be more guns around (her point) or a good thing because the NRA and its right-wing supporters would lose their influence (my point)? The content of the argument hardly matters. Neither of us had ever thought about plastic guns before. We were speculating, and then discussing, and then debating. making really good points, I told myself. I’m winning the debate. Through parry and thrust (in the language of fencing) I tried to take her down. To defeat her. All I really cared about was being right.
making really good points, I told myself. I’m winning the debate. Through parry and thrust (in the language of fencing) I tried to take her down. To defeat her. All I really cared about was being right. What I didn’t see until the next day was that Jane was hurt. She perceived my arguments as weapons — and indeed they were. I had thought: given competing positions, someone’s going to win, and that’s going to be me. She had thought: why is he putting me down? Why is he trying to cast my opinions as groundless and stupid?
What I didn’t see until the next day was that Jane was hurt. She perceived my arguments as weapons — and indeed they were. I had thought: given competing positions, someone’s going to win, and that’s going to be me. She had thought: why is he putting me down? Why is he trying to cast my opinions as groundless and stupid? going about it? Do I really want to change the minds of people steeped in medical thinking, addicts who believe they’re ill, their families, their doctors? Or do I just want to win a debate?
going about it? Do I really want to change the minds of people steeped in medical thinking, addicts who believe they’re ill, their families, their doctors? Or do I just want to win a debate? So I’m watching Matt facilitate a SMART meeting in Boston last night. SMART sometimes construes itself as “the alternative to AA.” SMART offers psychological tools, such as focusing on one’s own thought patterns and beliefs, and the potential that offers for behaviour change, even by small increments. SMART lends itself to mindfulness practices, it neither shames nor exonerates those who’ve “relapsed.” It is inclusive, it does its best to avoid dogma. And it values honesty and fellowship — as does its sometimes querulous cousin, AA.
So I’m watching Matt facilitate a SMART meeting in Boston last night. SMART sometimes construes itself as “the alternative to AA.” SMART offers psychological tools, such as focusing on one’s own thought patterns and beliefs, and the potential that offers for behaviour change, even by small increments. SMART lends itself to mindfulness practices, it neither shames nor exonerates those who’ve “relapsed.” It is inclusive, it does its best to avoid dogma. And it values honesty and fellowship — as does its sometimes querulous cousin, AA. thinking habits, to see their substance use more rationally, more comprehensively. But more than that, he was listening carefully to what people said and grasping what they were feeling: their fears, vulnerabilities, and their (often tattered) self-esteem.
thinking habits, to see their substance use more rationally, more comprehensively. But more than that, he was listening carefully to what people said and grasping what they were feeling: their fears, vulnerabilities, and their (often tattered) self-esteem.