
Hi you guys!!!!! Okay, I give up. I was seriously considering ending the blog, at least for a while. It’s time consuming! Especially trying to reply to your thoughtful and heart-felt comments. (I know I don’t have to, but I usually just feel like it.) I have two courses to teach in the next four months, and then there’s that book that’s supposed to be completed by June. Although my publishers may be somewhat flexible, I do want to finish by June. It’s a hot topic now. It may not be so hot in a couple of years.
The fact is, I miss you. I miss my blog, which means I miss communicating with you, my readers. It feels like a chunk removed from my life. And although there are a lot of other things I can attend to, I have learned a tremendous amount from this blog. About addiction and treatment and recovery and suffering and courage and being human and hurting deep down and soothing that hurt…and finding other ways to soothe it, other ways to feel. I don’t want to lose that incomparable source of knowledge, wisdom, compassion…whatever it is. I continue to study, write, and give talks about addiction and recovery. I’d better keep learning what I can about how it works. But beyond that, I just want to stay in touch. Whether you’re a frequent commenter or a hovering spook, I’ve become attached. You’re a second family to me.
So…New Year’s Resolution: I’ll try to keep my posts shorter — each one doesn’t have to be an award-winning essay — and just send you tidbits of stuff that seem new and important to me and that you might appreciate learning about too. Since I seem to be a blogging addict, I can at least try some form of harm reduction.
So here’s the connection. Last week I went to Toronto to give a keynote talk at the annual conference of the Ontario Harm Reduction Distribution Program. What an eye-opener! I thought I knew something about harm reduction. That’s when nice people try to keep addicts alive and relatively healthy until they can quit, right? Not 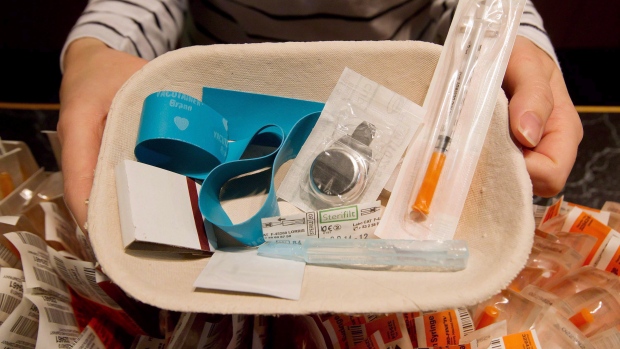 exactly. Here’s a cool radio piece about a harm reduction initiative in Amsterdam: supplying beer to serious alcoholics as partial payment for cleaning up the park they trashed the night before. Maybe this tells an important part of the story.
exactly. Here’s a cool radio piece about a harm reduction initiative in Amsterdam: supplying beer to serious alcoholics as partial payment for cleaning up the park they trashed the night before. Maybe this tells an important part of the story.
Well yes, harm reduction includes all that. But it’s also an entirely different approach to addiction, maybe you’d even call it a distinct philosophy. It doesn’t seem to have much to do with abstinence, for a start. Well, here’s how it came across to me. There were a couple of hundred people at this conference, and they make their living caring about people who most of society would prefer to write off. They seem to have unusually big hearts, and weird ideas to go with them. For example, teaching methamphetamine addicts to inject safely. How can you inject meth safely? The few times I shot meth, back in my chaotic twenties, I had no doubt that I was playing with death. One woman, a harm-reducer from London, Ontario, said, during her presentation: “We’ve distributed two million, one hundred and something thousand syringes this year. And we’re very proud of that.” Proud? I was shell-shocked. Proud? And when I passed the registration desk on day one, I was asked to try on the tourniquet. Arm-band, you mean, right? Isn’t it a nice navy blue color? And see how snugly it fits….velcro, you know.
I happened to be with my 25-year-old daughter that day. Still, as instructed, I pulled the thing around my upper arm, and sure enough those nearly-forgotten habits popped up to the surface of my consciousness, just as my veins popped up to the surface of my forearm. Besides being incredibly embarrassed in front of my daughter, who knows something of my history, I was simply grossed out. I haven’t shot drugs for over thirty years. Like is this some clever version of a registration tag, a door prize, or what? I couldn’t do it. Not that they were offering anything to go with it. But…it’s been too long. It was just yucck.
In keeping with my Resolution, I’ll end here. More on the conference, and some very interesting individuals I met there, next post.
Meanwhile, welcome back. And thanks for sticking around.
Leave a Reply to Donnie Mac Cancel reply